
Introduction
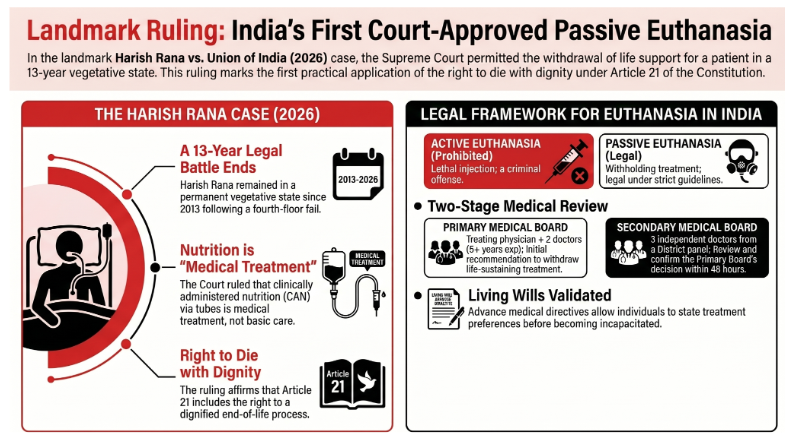
In the landmark case of Harish Rana vs Union of India (2026), the Supreme Court of India permitted the country’s first court-approved implementation of passive euthanasia. The ruling allows for the withdrawal of life-sustaining treatment for a patient in a permanent vegetative state (PVS), marking the first practical application of the 2018 Common Cause judgment which recognized the right to die with dignity under Article 21 of the Constitution.
Critical takeaways from this ruling include the legal classification of Clinically Administered Nutrition (CAN) as "medical treatment" rather than basic care, the waiver of mandatory waiting periods to prevent unnecessary suffering, and a stern directive to the Union Government to enact comprehensive end-of-life legislation. The Court emphasized that while passive euthanasia is now legally accessible under strict safeguards, India requires a robust palliative care infrastructure to ensure that financial distress or socio-economic vulnerability does not unfairly influence end-of-life decisions.
The Harish Rana Case (2026): A Judicial Turning Point
Case Background
Harish Rana, a 32-year-old man, had been in a Permanent Vegetative State (PVS) for over 13 years following a fall from a fourth-floor building in 2013. The accident resulted in catastrophic brain injuries and 100% quadriplegia. Since the accident, Rana was sustained solely through Clinically Assisted Nutrition and Hydration (CANH) via percutaneous endoscopic gastrostomy (PEG) tubes.
Supreme Court Observations and Ruling
The Supreme Court overturned a 2024 Delhi High Court dismissal of the family's plea, issuing the following directives:
Approval of Withdrawal: The Court accepted the unanimous recommendation of medical boards and the family to withdraw life support.
Palliative Care Integration: Harish Rana was ordered to be admitted to the palliative care department of AIIMS, Delhi, to undergo a "robust, palliative, and end-of-life care plan."
Humane Execution: The Court emphasized that withdrawal must manage pain and symptoms to ensure dignity and must not constitute "abandonment" of the patient.
Legal Status of CAN: The Court held that Clinically Administered Nutrition (CAN) via PEG tubes is "medical treatment." Consequently, its withdrawal falls under the scope of passive euthanasia and can be approved if it is no longer in the patient's best interest.
Procedural Expediency: The Court waived the standard 30-day reconsideration period to mitigate further suffering for the patient.
Legal and Statutory Framework in India
The Indian legal system draws a sharp distinction between different forms of euthanasia, primarily shaped by Supreme Court jurisprudence rather than specific legislation.
Classifications of Euthanasia
Active Euthanasia: A deliberate act (e.g., lethal injection) to cause death. This remains prohibited under the Bharatiya Nyaya Sanhita (BNS), 2023, and is treated as culpable homicide or murder.
Passive Euthanasia: Withholding or withdrawing life-sustaining treatment to allow a natural death. This is legal under strict safeguards.
Voluntary vs. Non-voluntary: Passive euthanasia can be voluntary (based on the patient's consent) or non-voluntary (performed when the patient is incompetent, such as in a coma).
Judicial Evolution
Case | Year | Core Ruling |
Maruti Shripati Dubal v. State of Maharashtra | 1987 | The Bombay High Court initially ruled the right to die was part of Article 21. |
Gian Kaur v. State of Punjab | 1996 | The Supreme Court reversed earlier logic, stating the right to life does not include the right to die. |
Aruna Shanbaug v. Union of India | 2011 | The SC permitted passive euthanasia under strict legal/medical safeguards for the first time. |
Common Cause v. Union of India | 2018 | The SC recognized the "right to die with dignity" and legally validated "Living Wills." |
Procedural Safeguards and Living Wills
To prevent abuse, the Supreme Court has established a two-stage medical review process for passive euthanasia, which was further streamlined in 2023 and 2026.
The Review Process
Primary Medical Board: Formed by the hospital; consists of the treating physician and two independent doctors with at least five years of experience.
Secondary Medical Board: Comprises three independent doctors from a panel maintained by the District Medical Officer.
Judicial Oversight: Decisions must be communicated to the Judicial Magistrate First Class (JMFC). Boards are encouraged to provide opinions within 48 hours.
Living Wills (Advance Medical Directives)
A Living Will is a written document allowing a person to provide explicit instructions regarding medical treatment in the event they become terminally ill or incompetent to consent. It authorizes families to switch off life support if medical boards declare the patient is beyond help.
Ethical and Social Dimensions: The Debate on Legalization
The debate surrounding euthanasia in India involves complex considerations of autonomy, medical ethics, and social vulnerability.
Category | Arguments in Favor | Arguments Against |
Autonomy & Rights | Fundamental right to self-determination and control over one's body. | No recognized "right to be killed"; Right to Life does not demand intentional termination. |
Compassion | Provides a merciful end to prolonged, unbearable agony. | Modern palliative care can effectively alleviate most suffering. |
Dignity | Permits a controlled, peaceful exit rather than forced endurance of low-quality life. | Risks devaluing the lives of the disabled or elderly as "not worth living." |
Regulation | Strict criteria and medical opinions can prevent abuse. | The "Slippery Slope" may lead to involuntary euthanasia or use for non-terminal mental illness. |
Burden | Reduces emotional and financial strain on families and society. | Pressure on vulnerable people to choose death to avoid being a "burden." |
Medical Ethics | Aligns with the duty to relieve suffering in hopeless cases. | Contradicts the Hippocratic Oath ("do no harm") and erodes patient trust. |
Strategic Recommendations for Terminally Ill Support
The Supreme Court urged the Union Government to enact a comprehensive law on end-of-life care to protect against outcomes shaped by financial distress or lack of insurance. The following pillars are identified for a better support system:
1. National Palliative Care Mission
Launch a dedicated mission to train healthcare workers and establish pain relief clinics in every district.
Ensure the availability of essential drugs, such as oral morphine, for chronic pain management.
2. System Integration and Financial Protection
Integrate palliative care across all levels of healthcare (PHCs to district hospitals).
Incorporate outpatient and home-based hospice care into Ayushman Bharat (PM-JAY) and the Ayushman Vay Vandana Scheme for senior citizens.
3. Community and Technology Support
Caregiver Models: Provide home care training and psychological counseling for families, replicating models like Kerala’s Neighbourhood Network in Palliative Care.
Digital Tools: Expand tele-palliative care for rural areas via Ayushman Arogya Mandirs and monitor patient outcomes through the Pradhan Mantri Ayushman Bharat Health Infrastructure Mission.
4. Legal Literacy
Conduct mass awareness campaigns regarding Living Wills.
Employ trained "patient advocates" in hospitals to facilitate end-of-life discussions with families.
Conclusion
The Harish Rana case represents a significant evolution in Indian jurisprudence, balancing the "right to die with dignity" with the necessity for strict medical oversight. However, the Court's warning remains clear: without comprehensive legislation and a universal palliative care system, the implementation of passive euthanasia remains vulnerable to socio-economic pressures.